


When I graduated I wanted to help people, and needed to KNOW that I was giving the right care and getting the best outcomes. How could I know this? Quite simply, this question drove me to search for and develop the corrective care model. To KNOW how much, how long, and how frequently to adjust a patient, and be absolutely certain of my own integrity, I had to validate the changes I set out to make. I began taking post x-rays after varying intervals and frequencies of intensive care, and meticulously recording outcomes for a full spectrum of patients. Through this process I discovered basic principles that would define my 30 plus years of practice and now help many other doctors do the same. This is the corrective care model: Prescribe specifically needed care at the outset for any given patient to produce maximum benefit; Direct the patient through the course of care to expected outcomes; Know on x-ray what is fixable, patchable, and unchangeable. Use of this model proved that most degeneration is avoidable, and chiropractic when applied correctly is the most gentle, simple, and powerful health care system in the world, NOT a system of pain control.
Basically, corrective care chiropractic is an approach to achieving and maintaining optimal health. The corrective doctor evaluates spinal condition and function as it affects the nervous system and seeks to OPTIMIZE IT. The alteration of biomechanics has PROFOUND influence on future health potential. Left uncorrected, remodeling of protective structures will instead forever diminish the CNS’s ability to function. Our CNS controls every cell tissue and organ making function at 100% of potential crucial.
On a patient’s first visit two basic forms of chiropractic care explained: general chiropractic and corrective care. General chiropractic focuses on relief of symptoms, while corrective care focuses on underlying structural abnormalities (that may be causing pain), and could be likened to spinal orthodontics. Although all chiropractors are able to give relief care, the corrective care chiropractor is a specialist, and will search for underlying causes of any health condition as it relates to the spine. Initially a specific plan is designed for each patient and, like the application of braces, adjustments will in time optimize biomechanics and nerve function. To the extent that this is realized, corrective care will arrest osteo-degenerative decay. In the most severe cases of pre-existing spinal degeneration, decay may only slow considerably, even with the best care. This is the unique potential that a corrective care approach affords requiring that adequate visits over a period of time are prescribed. Correction does not employ braces to hold or force the spine, instead maximizing the body’s neurological self-righting ability. This builds a healthier body and immune system, promotes an individual’s quality of life, and avoids needless suffering and damage.
As in dental orthodontics, patients invested in long term results naturally seek to maintain achieved gains. From this same perspective, children raised with regular chiropractic checkups will not have degenerative problems to overcome in adulthood. To a corrective care specialist, it makes no sense to wait and allow a child to develop problems before seeking care. Likewise, its futile to correct a problem then allow dysfunction and decay to take hold once more, and we discourage it! The corrective approach is clearly not suitable for patients looking for a “quick fix”, or for families not invested in life long health. This distinction is made clear from the outset, allowing the patient to choose their care freely. Likewise, making clear the consequences of leaving biomechanics uncorrected is an ethical duty of the doctor.
The Road To Recovery:
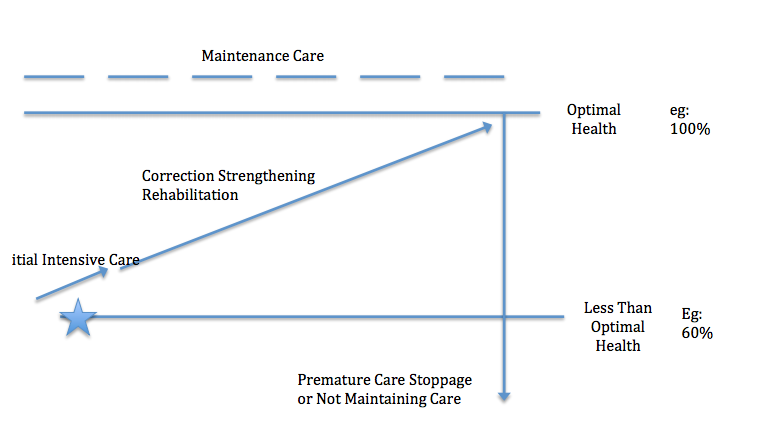
A visual model of corrective care The graph shows a starting point (the star) determined by detailed history, full spine evaluation, and standing weight bearing full spine X-Rays. This patient is at roughly 60% of her health potential, indicated on the right side of the graph. The first arrow up from the star indicates an initial period of intensive care addressing an acute presentation. Length of time and frequency will vary or be omitted based on individual needs. The next arrow up shows the course of corrective care adjustments. Optimal frequency to overcome inertia of chronically altered patterns is three times a week; the length of this period is determined by the individual’s condition. At the top right is conversion from corrective to maintenance care. Post x-rays are taken, any necessary exams repeated validating maximal correction, and adequate maintenance is determined. Ongoing monitoring during correction and maintenance is done via re-exams. Future checkups and x-rays validate that maintenance care frequency is sustaining correction. The vertical arrow extending from the right corner down to the bottom shows inevitable decline that occurs when care is stopped, or not adequately maintained. I have been startled to witness how quickly pre-existing degeneration takes hold and resumes when left unattended.
A 48 year old female with intermittent neck pain and headaches starting at the age of 18 years old to present is seen. History revealed she was in a motor vehicle accident at 18, was never treated chiropractically or otherwise as she believed “she was fine”. Her spine has degenerated at specific levels for almost 30 years since the initial accident. Generally on XRay 30% to 40% disc degeneration will be seen in the lower cervical spine with osteofitic poliferation (spurring), with similar X-Ray findings in the thoracic and lumbar spine if involved in the initial mechanism of injury. This example does not consider other traumas commonly suffered in 30 yars of life, making infinite variability with each patient the reason “typical” age based assumptions about the spine are useless. A carefully collected, and complete set of data is vital to avoid the prescription of too little or too much care. The most common mistake of an inexperienced doctor is to prescribe Initial Intensive Care Correction Strengthening Rehabilitation Maintenance Care Optimal Health Less Than Optimal Health Premature Care Stoppage or Not Maintaining Care eg: 100% Eg: 60% TOO LITTLE care. Tragically, this puts the patient at risk for avoidable degeneration, undermines optimal results, and ultimately the patient’s confidence in CHIROPRACTIC AS A WHOLE.
With my technique, it would take easily 6 to 8 months of three times per week for this now very chronic condition to stabilize. The patient is told clearly that at best, we hope to stop (or at least slow down) the degenerative process, thereby minimizing her future symptoms and loss of function. It is crucial for the doctor to not talk about her pain going away. I have never found patients with this amount of spinal and disc degeneration to be completely pain free for any long durations of time. This is the truth. Amongst ourselves as chiropractors, even if we have used chiropractic as I have, weekly checks and adjusted when necessary for the last 40 years, we know this does not afford me a pain free life!
With this realization, the crucial difference between the two basic approaches is exposed. A pain relief chiropractor will say “you’ll feel better under care” while a corrective care chiropractor will say “degeneration is not fixable, however its possible to slow, or even prevent future degeneration by stabilizing the subluxation.” Patients routinely feel much better under both kinds of care, however the focus and goal of care is radically different. We all know when a patient is told they will feel better and they DO à they often stop any further chiropractic care. In the patient’s mind, the goal has been achieved! We also know when a patient is told they’ll feel better under care and they DON’T à they often stop any future chiropractic care! In the patient’s mind the goal was not achieved, and chiropractic “didn’t work”! Either way the patient will never go on to experience long term benefits or even know these benefits exist! Given the choice many patients will choose correction, and some will not, however the outcomes must be known and agreed upon in the doctor patient relationship, not haphazardly assigned to the success or failure of chiropractic as a whole. To say that chiropractic does not work makes no more sense than blaming a general dentist for still having an overbite once a cavity is filled! Unfortunately, this is exactly why I believe chiropractic care is not mainstream today, any more than it was 30 years ago.
After almost 30 years I believe that the use of the road to recovery to explain corrective care is the best way for patients to make an informed decision and fully experience chiropractic. When I demonstrate real value people are more than happy to pay for the care they need. Now the doctor can work for the patient with no selling, no gimmicks, and no dealing with insurance. It is not only thoroughness of care that is needed for the best outcomes, its the patients understanding, election, and commitment to the same path. For this to occur there must be a commitment from the doctor to excellence, transparency, and an expert level of communication with the patient.
In other words, do what’s right because its right. You’ll sleep much better at night. You will enjoy practice and life much more. This is what I hope for all doctors and patients alike. The world truly needs what you alone as a chiropractor have the ability to give.
Chiropractically Yours, Jon Baker, D.C. Dr.
![]()
About the Author:
 Jon Baker graduated from Palmer College of Chiropractic in Davenport, Iowa in June of 1985. He started his first practice in Modesto, California in July of 1985 and consequentially opened 10 more satellite locations by 1996. In 1998 he started teaching other Chiropractors his methods and formed New Beginnings Chiropractic & Life Coaching. He retired from active practice in 2015 to go on a mission to save Chiropractic. More information may be found at www.chiropracticlifecoaching.com
Jon Baker graduated from Palmer College of Chiropractic in Davenport, Iowa in June of 1985. He started his first practice in Modesto, California in July of 1985 and consequentially opened 10 more satellite locations by 1996. In 1998 he started teaching other Chiropractors his methods and formed New Beginnings Chiropractic & Life Coaching. He retired from active practice in 2015 to go on a mission to save Chiropractic. More information may be found at www.chiropracticlifecoaching.com




{kind=link}