


Author: Kevin A. Kirby, DPM
Underscoring the potential ramifications of plantar fasciotomy procedures and plantar fascia ruptures, this author offers a closer look at 10 biomechanical functions of the plantar fascia, ranging from enhanced resupination of the subtalar joint during propulsion to reduced tension forces within the plantar ligaments, and reduced ground reaction force on metatarsal heads during late midstance and propulsion.
Given that the plantar fascia spans all the joints of the foot other than the digital interphalangeal joints, it has many important biomechanical functions that are critical to the normal function of the foot and lower extremity. Unfortunately, over the last three decades, surgeons have increasingly advocated plantar fasciotomy as a treatment for common foot pathologies such as plantar fasciitis without always giving full consideration to the potential problems that may occur over time with surgical release of the plantar fascia. 1-10
Patients who suffer from partial or complete plantar fascial ruptures may develop new symptoms and pathologies, some of which may be irreversible due to the loss of integrity of the plantar fascia and its important biomechanical functions.11-19 Given the importance of the intact plantar fascia for normal biomechanical function of the foot and lower extremity, it is critical for all foot healthcare specialists, especially foot surgeons, to fully understand the 10 functions of the plantar fascia first described more than two decades ago. 20
 1. Stiffening Medial And Lateral Longitudinal Arches And Reducing Longitudinal Arch Flattening
1. Stiffening Medial And Lateral Longitudinal Arches And Reducing Longitudinal Arch Flattening
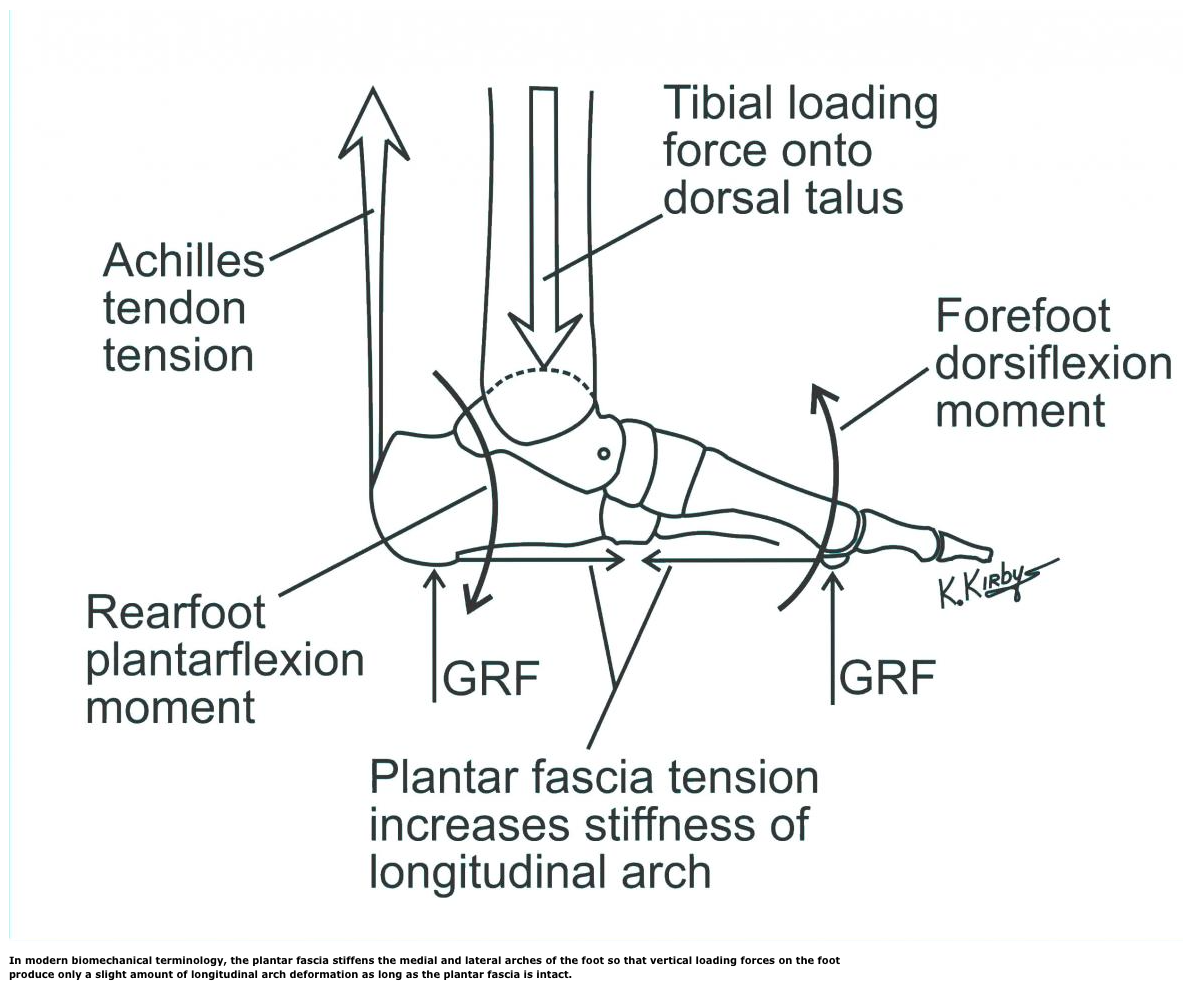
One of the first descriptions of the plantar fascia functioning to support the longitudinal arches of the foot and help prevent arch flattening came from Lapidus in 1943 when he modeled the longitudinal arch of the foot as a truss.21 He described the truss as consisting of two beams and a horizontal tie connecting the ends of the beams to help prevent the arch of the truss from deforming under vertical loading forces. Hicks further explored the longitudinal arch supporting function of the plantar fascia.22-25 He also described the truss function of the foot and how the two compression-bearing beams, consisting of the bones of the rearfoot and forefoot, along with a plantarly located tension-bearing tie, the plantar fascia, prevented elongation and flattening of the longitudinal arches under weightbearing loads.22-25
Scientific research on cadaver feet under simulated weightbearing forces has experimentally verified the basic mechanical concept of the truss mechanism of the longitudinal arch of the foot.26-32 Studies have demonstrated that sectioning of the plantar fascia not only lowers and elongates the medial and lateral longitudinal arches, but also increases dorsiflexion of the first metatarsal.26-32 Put in more modern biomechanical terminology, the plantar fascia stiffens the medial and lateral arches of the foot so vertical loading forces acting on the foot produce only a slight amount of longitudinal arch deformation as long as the plantar fascia is intact. However, loss of plantar fascial integrity by cutting or rupturing the plantar fascia will decrease the stiffness of the longitudinal arch, causing more longitudinal arch flattening for a given load.33
 2. Assisting In Resupination Of The Subtalar Joint During Propulsion
2. Assisting In Resupination Of The Subtalar Joint During Propulsion
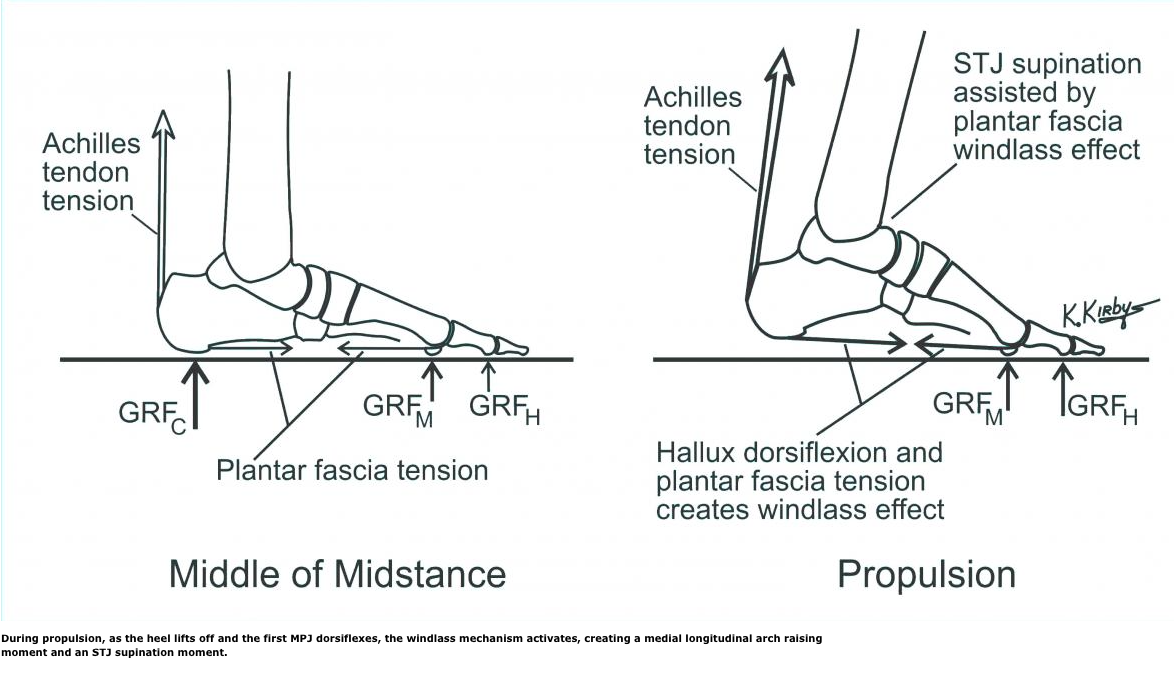
In 1954, Hicks first described his experimental observation that hallux dorsiflexion produced longitudinal arch raising of the foot in both cadaver feet and in live subjects using the mechanical analogy of a windlass.22 He noted that dorsiflexion of the hallux not only raised the longitudinal arch but also supinated the subtalar joint (STJ) and externally rotated the leg. The arch raising effect of hallux dorsiflexion nearly completely disappeared with complete transection of the plantar fascia in cadaver feet. The author noted that the arch raising mechanism of hallux dorsiflexion occurred “without the direct action of any muscle.”
During propulsion, as the heel lifts off and the first MPJ dorsiflexes, the windlass mechanism activates, creating a medial longitudinal arch raising moment and an STJ supination moment. The gastrocnemius and soleus muscles also exert contractile activity during propulsion. This increases the tension force within the Achilles tendon, which passes medial to the STJ axis. The resultant Achilles tendon tension during propulsion will cause an STJ supination moment, which helps cause STJ supination during propulsion. Therefore, STJ supination moments caused by hallux dorsiflexion during propulsion due to the windlass mechanism assist the gastrocnemius and soleus muscles in causing normal STJ supination motion during propulsion.34
Ward and colleagues confirmed the ability of the plantar fascia to assist in resupination of the STJ during propulsion in a novel experiment that utilized a dynamic gait replicator.35 This allowed a cadaver foot to “walk” through the attachment of servomotors to the extrinsic muscles of the cadaver foot. The authors’ experiments involved progressive sectioning of the plantar fascia, from medial to lateral, to determine the biomechanical effects of progressive plantar fasciotomy. They found that before sectioning the plantar fascia, the cadaver feet resupinated normally during propulsion. However, as the plantar fascia was sectioned progressively from medial to lateral, STJ supination lessened, supporting the idea that the plantar fascia assists in STJ supination during propulsion.
3. Assisting Deep Posterior Compartment Muscles By Increasing The Subtalar Supination Moment
During walking gait, the deep posterior compartment muscles (i.e., posterior tibial, flexor digitorum longus and flexor hallucis longus muscles) are active during the early and latter part of the stance phase.36 Since all of the tendons of the deep posterior compartment muscles pass medial to the STJ axis, they will all exert a STJ supination moment. This moment will tend to decelerate STJ pronation during the early stance phase and accelerate STJ supination during the latter half of stance phase.37
Since the plantar fascia stiffens the medial longitudinal arch of the foot, helping to prevent excessive dorsiflexion of the medial column of the foot, it will also help stabilize the medial longitudinal arch against excessive STJ pronation motion.38-40 In effect, the plantar fascia acts to prevent excessive STJ pronation motion during the stance phase of walking by increasing the stability of the medial column under weightbearing loads. By stiffening the medial column, the plantar fascia may indirectly cause an STJ supination moment since it functions to help resist STJ pronation motion.33 Therefore, since the muscles of the deep posterior compartment increase the internal STJ supination moment and the plantar fascia indirectly causes a STJ supination moment during stance, by definition, we can think of the plantar fascia as assisting the deep posterior compartment muscles in the production of STJ supination moment during stance.
 4. Assisting Plantar Intrinsic Muscles To Prevent Flattening Of The Medial Longitudinal Arch
4. Assisting Plantar Intrinsic Muscles To Prevent Flattening Of The Medial Longitudinal Arch
The plantar intrinsic muscles of the foot are active in the latter half of midstance and throughout the propulsive phase of walking gait.41-43 The plantar intrinsic muscles that insert either directly or indirectly onto the proximal phalanges of the digits all have the potential — by increasing the posterior directed compression force on the metatarsal heads — to stiffen the longitudinal arch of the foot, and help prevent longitudinal arch flattening.44,45
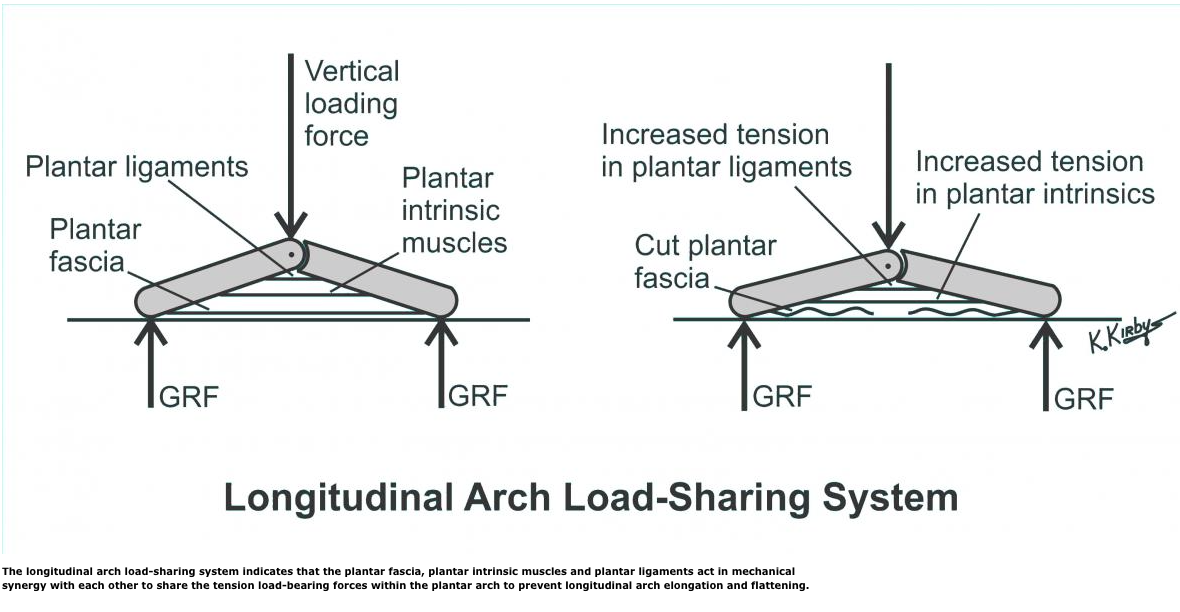
As I noted earlier, researchers have demonstrated that the plantar fascia increases the stiffness of the medial longitudinal arch of the foot.26,27,29,39,46,47 This results in the plantar fascia helping to resist medial longitudinal arch flattening when the ground reaction force (GRF) acts on the plantar surface of the foot. Since the plantar fascia and the larger plantar intrinsic muscles share similar anatomic locations within the plantar foot, they will share biomechanical functions by exerting tension-loading forces plantarly across the joints of the foot to prevent elongation and flattening of the longitudinal arch. In addition, since the plantar ligaments of the STJ, midtarsal and midfoot joints all help prevent flattening of the longitudinal arch, we can think of them as all sharing biomechanical functions with each other.
In order to better explain the mechanical interrelationship of the tension load-bearing structures of the longitudinal arch of the foot, Kirby has modelled the foot as having a longitudinal arch load-sharing system (LALSS).33 Under this system, the plantar fascia, plantar intrinsic muscles and plantar ligaments act in mechanical synergy with each other to share the tension load-bearing forces within the plantar arch to prevent longitudinal arch elongation and flattening. Failure of one of the structures of the LALSS, which would occur in a plantar fascia rupture or in a plantar fasciotomy, will increase the tension forces acting within both of the remaining plantar tension load-bearing structures, namely the plantar intrinsic muscles and plantar ligaments. However, during normal function, these plantar arch structures all work in harmony to maintain longitudinal arch height and stability during weightbearing activities.33
5. Reducing Tension Forces Within The Plantar Ligaments
The concept of the LALSS is based on the fact that the plantar fascia, plantar intrinsic muscle and plantar ligaments all work together to stiffen the longitudinal arch of the foot by sharing the tension loading forces. These forces are necessary to prevent longitudinal arch flattening and elongation. When the plantar fascia is cut or ruptured, the deepest layer of the LALSS, the plantar ligaments, will be subject to increased tension force since the plantar fascia is no longer performing its longitudinal arch supporting function.33
In support of this theory, Crary and coworkers found the average strain in the spring ligament increased by 52 percent and the average strain in the long plantar ligament increased by 94 percent after plantar fasciotomy.48 In addition, finite element analysis research studies have also shown that the plantar ligaments develop increased tension stresses after plantar fasciotomy.40,49,50 Therefore, the literature confirms that plantar fasciotomy and/or plantar fascia rupture increases the tension stress and strain within the plantar ligaments, and is consistent with the LALSS model of the foot.
 6. Preventing Excessive Dorsal Interosseous Compression Forces In Midtarsal And Midfoot Joints
6. Preventing Excessive Dorsal Interosseous Compression Forces In Midtarsal And Midfoot Joints
During normal weightbearing activities, the structural components of the longitudinal arch of the foot must develop sufficient internal forces to prevent longitudinal arch elongation and flattening. As I noted earlier, the LALSS contributes plantarly located tension forces to help prevent longitudinal arch flattening. However, the bones and joints of the longitudinal arch of the foot also develop internal forces that resist the compression and bending forces that are equally as important as the plantar tension forces of the LALSS in maintaining longitudinal arch integrity.
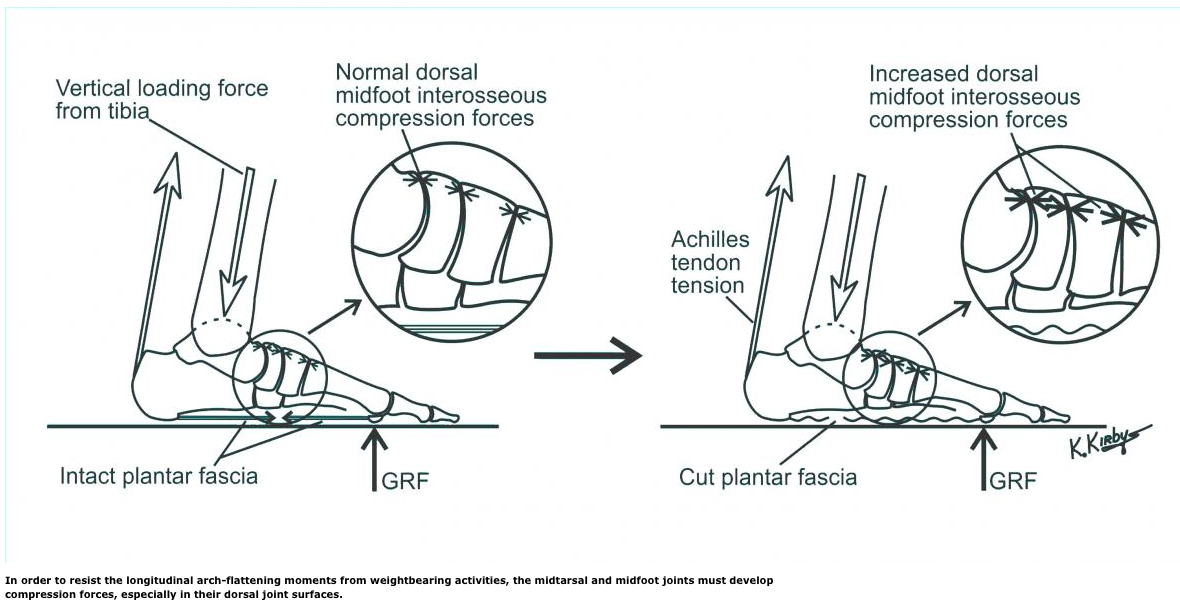
The combination of ground reaction force acting on the forefoot, Achilles tendon tension force and inferiorly directed tibiotalar loading forces during the stance phase of gait produces a significant longitudinal arch flattening moment. The longitudinal arch flattening moment is the result of ground reaction force acting on the forefoot, producing a forefoot dorsiflexion moment, Achilles tendon tension and an inferiorly directed tibiotalar compression force, which causes a rearfoot plantarflexion moment.51
In order to resist the longitudinal arch flattening moments from weightbearing activities, the midtarsal and midfoot joints must develop compression forces, especially in their dorsal joint surfaces. Loss of plantar fascial integrity will increase longitudinal arch flattening. This leads to further compression of the dorsal joint surfaces of the midtarsal and midfoot joints, which may lead to dorsal midfoot pain.9,29,52-56 Excessive dorsal midfoot joint compression forces may also result from increased longitudinal arch flattening forces and lead to the dorsal midfoot joint pain known as dorsal midfoot interosseous compression syndrome.57 Accordingly, by preventing dorsiflexion of the midtarsal and midfoot joints and longitudinal arch flattening, the plantar fascia will help prevent pathological levels of dorsal midtarsal joint and midfoot joint compression forces during gait.
 7. Preventing Excessive Dorsiflexion Bending Moments On Metatarsals
7. Preventing Excessive Dorsiflexion Bending Moments On Metatarsals
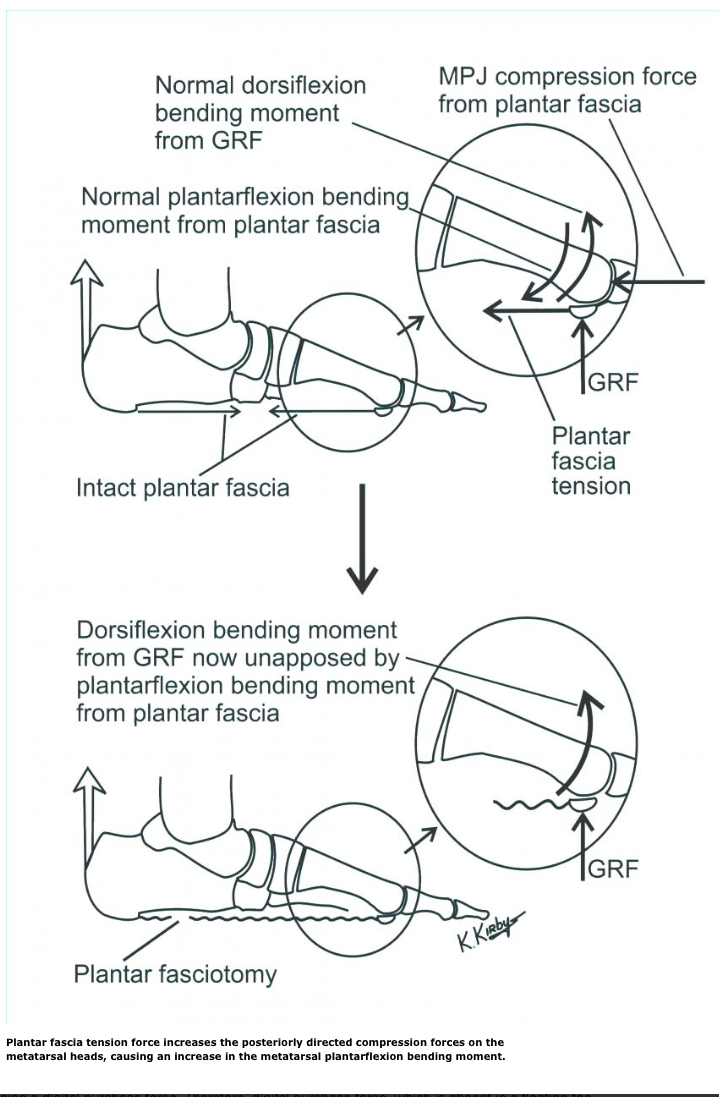
By way of its insertions onto the hallucal sesamoids and lesser MPJ plantar plates, and ultimately into the bases of the digital proximal phalanges, the plantar fascia also acts to prevent excessive dorsiflexion bending moments on the metatarsals. Plantar fascia tension force increases the posteriorly directed compression forces on the metatarsal heads, causing an increase in the metatarsal plantarflexion bending moment. A plantar fasciotomy or plantar fascia rupture will decrease the metatarsal plantarflexion bending moment, which will allow the metatarsal dorsiflexion bending moments from ground reaction force acting on the plantar metatarsal heads to increase the dorsiflexion bending of the metatarsals.58
Experimental studies on cadavers in simulated weightbearing conditions demonstrate that both dorsiflexion bending moments and dorsal metatarsal strains are greater with plantar fasciotomy.32,59 A 65 percent increase in dorsal metatarsal compression stresses after plantar fasciotomy was evident in a 2002 study.60 Other studies have shown similar increases in metatarsal stress with plantar fasciotomy.40,49,50,61 Authors have even cited stress fractures of the third metatarsal as a post-surgical consequence of endoscopic plantar fasciotomy.62
8. Passively Maintaining Digital Purchase And Stabilizing The Proximal Phalanx Of Digits In The Sagittal Plane
Due to its distal insertions onto the sesamoids, plantar plates and bases of the proximal phalanges of all five digits, the plantar fascia has the unique ability to maintain passive digital purchase force by effectively plantarflexing the digits into the ground. Loading of the plantar forefoot during weightbearing activities will dorsiflex the forefoot relative to the rearfoot, elongating the longitudinal arch and increasing the tension within the plantar fascia. This passive increase in the plantar fascia tension force increases the MPJ plantarflexion moment, which causes the digit to plantarflex into the ground, causing a digital purchase force. Therefore, digital purchase force, which is absent in a floating toe deformity, is directly due to the passive effects of plantar fascia tension and does not require active digital flexor muscle action to occur.63
In support of this idea, Sharkey and colleagues demonstrated a significant reduction in plantar digital pressure and plantar digital contact force with plantar fasciotomy of cadaver feet in simulated weightbearing conditions.32 The loss of the passively created plantar fascia tension force, which occurs with plantar fasciotomy, plantar fascia rupture or even in plantar plate rupture, reduces the proximal phalanx plantarflexion moment. This may ultimately lead to floating toe or hammertoe deformities, effectively decreasing the important weightbearing capabilities of the digits.64
9. Reducing Ground Reaction Force On Metatarsal Heads During Late Midstance And Propulsion
Due to the passive ability of the plantar fascia to increase the MPJ plantarflexion moments and thereby increase the digital purchase force, the plantar fascia also acts to reduce the plantar loading forces on the metatarsal heads during late midstance and propulsion. The digital purchase force that results from the increase in plantar fascia tension during late midstance and propulsion will allow the plantar digits to share the plantar forefoot load with the metatarsal heads, specifically reducing the ground reaction force on the metatarsal heads.63,65
Sharkey and coworkers demonstrated that progressive transection of the plantar fascia in cadaver feet in simulated weightbearing conditions caused significant increases in plantar pressure and plantar ground reaction force at the metatarsal heads.32 The authors thought this was directly caused by the decrease in digital force from loss of tension forces within the plantar fascia. Therefore, the integrity of the plantar fascia is essential to prevent excessive loading forces on the metatarsal heads, which may lead to painful conditions of the plantar forefoot, such as plantar plate tears and metatarsalgia.
10. Helping Absorb And Release Elastic Strain Energy During Running
Wright and Rennels first demonstrated the elastic properties of the plantar fascia, and that the plantar fascia elongated under increased tension loading and returned to its original length with decreased tension loading.66 In addition, a classic experiment by Ker and coworkers on a cadaver foot subjected to cyclical loading forces that simulated running showed that the plantar ligaments and plantar fascia stored and released 17 Joules of elastic strain energy, and the Achilles tendon stored and subsequently released 35 Joules of elastic strain energy with each loading cycle of the longitudinal arch of the foot.38 Their conclusion was that “the arch of the foot stores enough strain energy to make running more energy efficient.”
Humans are not the only animals to store significant amounts of elastic strain energy within their ligaments and tendons during locomotor activities. In wallabies, 33 percent of the work done during slow hopping occurs via the long tendons in their hind limbs, which first stretch and then recoil to release elastic strain energy during hopping.67 Horses also store elastic strain energy within the long tendons of their forelimbs and hind limbs, which allows them to save an estimated 20 to 40 percent of the mechanical work during walking, trotting and galloping.68 Therefore, like other running animals, the bipedal human has the ability to store and release a significant amount of elastic strain energy within the plantar fascia that makes running, and possibly other locomotor activities, a more metabolically efficient activity.
In Conclusion
The plantar fascia is a vitally important structure of the foot that has multiple biomechanical functions. These functions are critical in allowing normal foot and lower extremity function during the numerous weightbearing activities that individuals perform during their daily lives. Plantar fasciotomy or plantar fascial rupture may cause significant negative biomechanical effects that may, over time, lead to new symptoms, pathologies and deformities. With this in mind, in order to maximize the potential benefits and minimize the potential complications from plantar fasciotomy, and in order to better appreciate the potential clinical sequelae of plantar fascial rupture, the podiatric surgeon should fully understand the ten biomechanical functions of the plantar fascia.

Dr. Kirby is an Adjunct Associate Professor within the Department of Applied Biomechanics at the California School of Podiatric Medicine at Samuel Merritt University in Oakland, Calif. He is in private practice in Sacramento, Calif.
References
- Barrett SL, Day SV, Brown MG. Endoscopic plantar fasciotomy: preliminary with cadaveric specimens. J Foot Surg. 1991; 30(2):170–172.
- Barrett SL, Day SV. Endoscopic plantar fasciotomy: two portal endoscopic surgical techniques: Clinical results of 65 procedures. J Foot Ankle Surg. 1993; 32(3):28-256.
- Graves RH, Levin DR, Giacopelli J, White PR, Russell RD. Fluoroscopy-assisted plantar fasciotomy and calcaneal exostectomy: A retrospective study and comparison of surgical techniques. J Foot Ankle Surg. 1994; 33(5):475-481.
- Barrett SL. Endoscopic planta fasciotomy. Clin Pod Med Surg. 1994; 11(3):469-481.
- Perelman GK, Figura MA, Sandberg NS. The medial instep plantar fasciotomy. J Foot Ankle Surg. 1995; 34(5):227-457.
- Barrett SL, Day SV, Pignetti TT, Robinson LB. Endoscopic plantar fasciotomy: A multi-surgeon prospective analysis of 652 cases. J Foot Ankle Surg. 1995; 34(4):400-406.
- Benton-Weil W, Borrelli AH, Weil LS, Weil LS. Percutaneous plantar fasciotomy: A minimally invasive procedure for recalcitrant plantar fasciitis. J Foot Ankle Surg. 1998; 37(4):269-272.
- Lundeen RO, Aziz S, Burks JB, Rose JM. Endoscopic plantar fasciotomy: A retrospective analysis of results in 53 patients. J Foot Ankle Surg. 2000; 39(4):208-217.
- Fishco WD, Goecker RM, Schwartz RI. The instep plantar fasciotomy for chronic plantar fasciitis. A retrospective review. J Am Podiatr Med Assoc. 2000; 90(2):66-69.
- Saxena A. Uniportal plantar fasciotomy: A prospective study on athletic patients. Foot Ankle Int. 2004; 25(12):882-889.
- Leach R, Jones R. Rupture of the plantar fascia in athletes. J Bone Joint Surg. 1978; 60(4):537-539.
- Ahstrom JP. Spontaneous rupture of the plantar fascia. Am J Sports Med. 1988; 16(3):306-307.
- Sellman JR. Plantar fascia rupture associated with corticosteroid injection. Foot Ankle Int. 1994; 15(7):376-381.
- Pai VS. Rupture of the plantar fascia. J Foot Ankle Surg. 1996; 35(1):39-40.
- Rolf C, Guntner P, Ericsater J, Turan I. Plantar fascia rupture: Diagnosis and treatment. J Foot Ankle Surg. 1997; 36(2):112-114.
- Acevedo JI, Beskin JL. Complications of plantar fascia rupture associated with corticosteroid injection. Foot Ankle Int. 1998; 19(2):91-97.
- Theodorou DJ, Theodorou SJ, Kakitsubata Y, Lektrakul N, Gold GE, Roger B, Resnick D. Plantar fasciitis and fascial rupture: MR imaging findings in 26 patients supplemented with anatomic data in cadavers. Radiographics. 2000; 20:s181-197.
- Saxena A, Fullem B. Plantar fascia ruptures in athletes. Am J Sports Med. 2004; 32(3):662-665.
- Kim C, Cashdollar MR, Mendicino RW, Catanzariti AR, Fuge L. Incidence of plantar fascia ruptures following corticosteroid injection. Foot Ankle Spec. 2010; 3(6):335-337.
- Kirby KA. Foot and Lower Extremity Biomechanics: A Ten Year Collection of Precision Intricast Newsletters. Precision Intricast, Inc., Payson, Arizona, 1997, pp. 45-46.
- Lapidus PW. Misconception about the ‘‘springiness’’ of the longitudinal arch of the foot. Arch Surg. 1943; 46:410–421.
- Hicks JH. The mechanics of the foot. II. The plantar aponeurosis and the arch. J Anat. 1954; 88(1):24-31.
- Hicks JH. The foot as a support. Acta Anatomica. 1955; 25(1):34-45.
- Hicks JH. The mechanics of the foot IV. The action of muscles on the foot in standing. Acta Anatomica. 1956; 27(3):180-192.
- Hicks JH. The three weight bearing mechanisms of the foot. In F.G. Evans (ed): Biomechanical Studies of the Musculoskeletal System. C.C. Thomas Co., Springfield, 1961, pp. 161-191.
- Huang CK, Kitaoka HB, An KN, Chao EY. Biomechanical evaluation of longitudinal arch stability. Foot Ankle Int. 1993; 14(6):353-357.
- Kitaoka HB, Luo ZP, Kai-Nan A. Effect of plantar fasciotomy on stability of arch of foot. Clin Ortho Rel Res. 1997; 344:307-12.
- Kitaoka HB, Luo ZP, An KN. Mechanical behavior of the foot and ankle after plantar fascia release in the unstable foot. Foot Ankle Int. 1997;18(1):8-15.
- Thordarson DB, Kumar PJ, Hedman TP, Ebramzadeh E. Effect of partial versus complete plantar fasciotomy on the windlass mechanism. Foot Ankle Int. 1997; 18(1):16-20.
- Sharkey NA, Ferris L, Donahue SW. Biomechanical consequences of plantar fascial release or rupture during gait: Part I – Disruptions in longitudinal arch conformation. Foot Ankle Int. 1998; 19(12):812-820.
- Murphy GA, Pneumaticos SG, Kamaric E, Noble PC, Trevino SG, Baxter DE. Biomechanical consequences of sequential plantar fascia release. Foot Ankle Int. 1998; 19(3):149-152.
- Sharkey NA, Donahue SW, Ferris L. Biomechanical consequences of plantar fascial release or rupture during gait. Part II: Alterations in forefoot loading. Foot Ankle Int. 1999; 20(2):86-96.
- Kirby KA. Foot and Lower Extremity Biomechanics IV: Precision Intricast Newsletters, 2009-2013. Precision Intricast, Inc., Payson, AZ, 2014, pp. 27-36.
- Kirby KA. Foot and Lower Extremity Biomechanics III: Precision Intricast Newsletters, 2002-2008. Precision Intricast, Inc., Payson, AZ, 2009, pp. 127-128.
- Ward ED, Smith KM, Cocheba JR, Patterson PE, Phillips RD. In vivo forces in plantar fascia during stance phase of gait. Sequential release of plantar fascia. J Am Podiatr Med Assoc. 2003; 93(6):429-442.
- Root ML, Orien WP, Weed JH. Normal and Abnormal Function of the Foot. Clinical Biomechanics Corp., Los Angeles, CA, 1977, pp. 203-213.
- Kirby KA. Rotational equilibrium across the subtalar joint axis. J Am Podiatr Med Assoc. 1989; 79(1):1-14.
- Ker RF, Bennett MB, Bibby SR, Kester RC, Alexander RM. The spring in the arch of the human foot. Nature. 1987; 325(7000):147-149.
- Arangio GA, Chen C, Kim W. Effect of cutting the plantar fascia on mechanical properties of the foot. Clin Ortho Rel Res. 1997; 339:227-231.
- Cheung JTM, Zhang M, An KN. Effects of plantar fascia stiffness on the biomechanical responses of the ankle-foot complex. Clin Biomech. 2004; 19(8):839-846.
- Sheffield FJ, Gersten JW, Mastellone AF. Electromyographic study of the muscles of the foot in normal walking. Am J Phys Med. 1956; 35(4):223-236.
- Mann R, Inman VT. Phasic activity of intrinsic muscles of the foot. J Bone Joint Surg. 1964; 46A:469-481.
- Gray EG, Basmajian JV. Electromyography and cinematography of leg and foot (“normal” and flat) during walking. Anat Rec. 1968; 161(1):1-15.
- Root ML, Orien WP, Weed JH. Normal and Abnormal Function of the Foot. Clinical Biomechanics Corp., Los Angeles, CA, 1977, pp. 228-250.
- Headlee DL, Leonard JL, Hart JM, Ingersoll CD, Hertel J. Fatigue of the plantar intrinsic foot muscles increases navicular drop. J Electromyo Kinesio. 2008; 18(3):420-426.
- Arangio GA, Chen C, Salathe EP. Effect of varying arch height with and without the plantar fascia on the mechanical properties of the foot. Foot Ankle Int. 1998; 19(10):705-709.
- Caravaggi P, Pataky T, Gunther M, Savage R, Crompton R. Dynamics of longitudinal arch support in relation to walking speed: contribution of the plantar aponeurosis. J Anat. 2010; 217(3):254-261.
- Crary JL, Hollis JM, Manoli A. The effect of plantar fascia release on strain in the spring and long plantar ligaments. Foot Ankle Int. 2003; 24(3):245-250.
- Cheung JT, An KN, Zhang M. Consequences of partial and total plantar fascia release: A finite element study. Foot Ankle Int. 2006; 27(2):125-132.
- Wu L. Nonlinear finite element analysis for musculoskeletal biomechanics of medial and lateral plantar longitudinal arch of Virtual Chinese Human after plantar ligamentous structure failure. Clin Biomech. 2007; 22(2):221-229.
- Kirby KA. Foot and Lower Extremity Biomechanics II: Precision Intricast Newsletters, 1997-2002. Precision Intricast, Inc., Payson, AZ, 2002, pp. 141-152.
- Sellmann JR. Plantar fascia rupture associated with corticosteroid injection. Foot Ankle Int. 1994; 15(7):376-381.
- Acevedo JI, Beskin JL. Complications of plantar fascia rupture associated with corticosteroid injection. Foot Ankle Int. 1998; 19(2):91-97.
- Yu JS, Spigos D, Tomczak R. Foot pain after a plantar fasciotomy: an MR analysis to determine potential causes. J Comput Assist Tomogr. 1999; 23(5):707-712.
- O’Malley MJ, Page A, Cook R. Endoscopic plantar fasciotomy for chronic heel pain. Foot Ankle Int. 2000; 21(6):505-510.
- Jerosch J. Endoscopic release of plantar fasciitis – a benign procedure? Foot Ankle Int. 2000; 21(6):511-513.
- Kirby KA. Foot and Lower Extremity Biomechanics: A Ten Year Collection of Precision Intricast Newsletters. Precision Intricast, Inc., Payson, Arizona, 1997, pp. 165-168.
- Kirby KA. Foot and Lower Extremity Biomechanics III: Precision Intricast Newsletters, 2002-2008. Precision Intricast, Inc., Payson, AZ, 2009, pp. 99-102.
- Donahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. 1999; 81(9):1236-1244.
- Gefen A. Stress analysis of the standing foot following surgical plantar fascia release. J Biomechanics. 2002; 35(5):629-637.
- Lian J, Y YF, Yu GR, Niu WX, Wang YB. Deformation and stress distribution of the human foot after plantar ligaments release: A cadaveric study and finite element analysis. Sci China Life Sci. 2011; 54(3):267-271.
- Sammarco GJ, Idusuyi OB. Stress fracture of the base of the third metatarsal after an endoscopic plantar fasciotomy: A case report. Foot Ankle Int. 1998; 19(3):157-159.
- Kirby KA. Foot and Lower Extremity Biomechanics III: Precision Intricast Newsletters, 2002-2008. Precision Intricast, Inc., Payson, AZ, 2009, pp. 103-110.
- Hamel AJ, Donahue SW, Sharkey NA. Contributions of active and passive toe flexion to forefoot loading. Clin Orthop Rel Res. 2001; 393:326-334.
- Erdimir A, Hamel AJ, Fauth AR, Piazza SJ, Sharkey NA. Dynamic loading of the plantar aponeurosis in walking. J Bone Joint Surg. 2004; 86A(3):546-552.
- Wright DG, Rennels DC. A study of the elastic properties of plantar fascia. J Bone Joint Surg. 1964; 46:482-492.
- Kram R, Dawson TJ. Review: Energetics and biomechanics of locomotion by red kangaroos (Macropus rufus). Comp Biochem Physio. 1998; 120(1):41-19.
- Biewener AA. Muscle-tendon stresses and elastic energy storage during locomotion in the horse. Comp Biochem Physiol. 1998; 120(1):73-87.
Additional Reference
69. Kelikian AS. Sarrafian’s Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, Third Edition. Lippincott Williams & Wilkins, Philadelphia, 2011, pp. 144-150




{kind=link}