

Submitted by Shawn Thistle, DC, of RRS Education
Study Title: “Systematic Review and Meta-Analysis of Chiropractic Care and Cervical Artery Dissection: No Evidence for Causation”
Authors: Church E, Sieg E, Zalatimo O, et al.
Publication Information: Cureus 2016; 8(2): e498. DOI:10.7759/cureus.498
Introduction
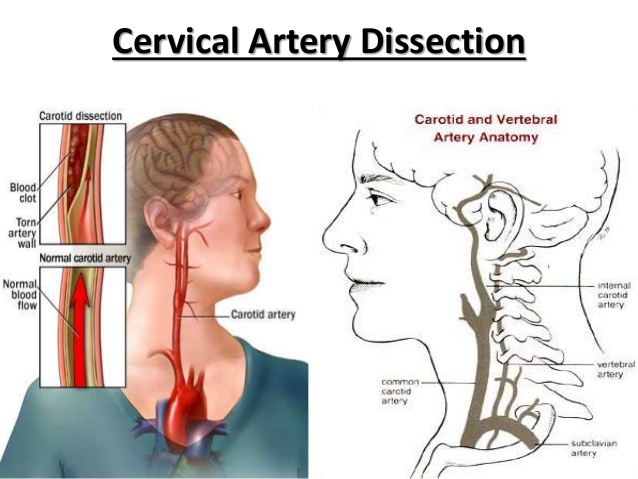
Based on case reports/series and case-control studies, an association between chiropractic neck manipulation (CM) and cervical artery dissection (CAD) has been proposed. However, questions remain as to whether CM is actually a cause of CAD, or if the relationship is the result of other extraneous factors.
Though millions of people receive CM each year, CAD is a rare occurrence with an annual incidence of approximately 2.5–3 cases per 100,000 in the population for internal carotid artery dissection and 1–1.5 per 100,000 for vertebral artery dissection.1
Chiropractic manipulation-related CAD cases have been publicized repeatedly, in part because the affected patients are often relatively young and in seemingly good health before the incident. Nonetheless, if CM is actually a cause of CAD, the condition could potentially be prevented.
The purpose of this study was to examine the strength of evidence about whether CM causes CAD by performing a systematic review, meta-analysis and evaluation of the body of evidence as a whole.
Pertinent Results
The database searches netted 253 articles, with 77 of them being judged as non-relevant. Four of the relevant articles were considered to be class III studies and only two were deemed class II. Sixty-three studies were considered to be class IV and were not included in the meta-analysis.
Although there were considerable differences between the outcomes of the included class II and III studies, a small association between dissection and chiropractic care was suggested, OR 1.74 (95% CI 1.26-2.41). When class III studies were excluded and the meta-analysis repeated, a small association between dissection and chiropractic care was still apparent, OR 3.17 (95% CI 1.30-7.74).
The GRADE rating of the quality of the body of evidence was determined to be very low due to the involved study designs being observational, the potential for bias and because the body of evidence was derived from measures of association.
Hill’s criteria for assigning causation to an association were used to determine the likelihood of causation between CM and CAD. There are nine Hill’s criteria, including strength of association, consistency, specificity, temporality, biological gradient, plausibility, coherence, experimental evidence and analogy. Only one of the nine criteria was clearly met, four were considered equivocal due to the absence of relevant data, and four failed to meet Hill’s requirements.
Clinical Application and Conclusions
The most impactful message presented in this paper is best captured in a quote from the authors themselves: “We found no evidence for a causal link between chiropractic care and CAD. This is a significant finding because belief in a causal link is not uncommon, and such a belief may have significant adverse effects such as numerous episodes of litigation.” There have been many case reports of this relationship and case-control studies have shown small associations between CM and CAD; however, the quality of the body of evidence is very low. Furthermore, because there is an association between neck pain and CAD, which leads patients to seek CM, there is a high risk of bias and confounding among the involved studies.
The authors indicated that cervical artery dissection is a rare event and CM has only been reported as being associated with CAD in 6% to 9% of cases.2 Thus, the possibility of a CAD occurring in association with CM is exceedingly rare. Nonetheless, when a patient suffers CAD in close proximity to CM, right or wrong, the practitioner may be blamed.
The best clinical strategy when performing CM is to be vigilant for signs and symptoms of CAD and when present do not perform CM; instead, refer the patient for appropriate medical care.3
Study Methods
A search of the Medline and Cochrane databases was conducted using the terms “chiropract*,” “spinal manipulation,” “carotid artery dissection,” “vertebral artery dissection” and “stroke.” Articles were included if they involved human trials that considered patients with carotid or vertebrobasilar artery dissection and recent CM. Articles that were not written in English were excluded.
Articles were reviewed independently by two of the study’s authors, who also independently rated the articles using the American Academy of Neurology’s classification of evidence scheme.4 Any discrepancies in rating the articles were arbitrated by a third author.
A meta-analysis of class II and class III studies was performed (higher class numbers point to lower quality). A second meta-analysis, which excluded class III studies, was also performed.
The quality of the total body of evidence was evaluated using the GRADE system, which rates evidence as high, moderate, low, or very low quality. In rating studies, the GRADE system considers study design, risk of bias, inconsistency, indirectness, imprecision, publication bias, effect size, dose response and all plausible residual confounding.
Study Strengths/Weaknesses
This was a well-done, unbiased review that fairly considered the relationship between CM and CAD. This appears to be especially true when one considers that the authors are affiliated with highly reputable neurosurgery centers.
The studies included in this review were generally of low quality. Even the better studies that comprised the meta-analysis acquired data from health administrative databases that may have included erroneous ICD coding leading to misclassification bias.
The authors indicated that the most significant threat to drawing firm conclusions from the studies in this review is that they only point to a correlation, not a causal relationship. Furthermore, a number of extraneous variables potentially confound this relationship. The most probable confounder is the fact that 80% of patients with CAD report symptoms of neck pain and/or headache and are therefore more likely to visit a chiropractor than patients without neck pain.
Dr. Thistle is a practicing chiropractor, educator, international speaker, knowledge-transfer leader, entrepreneur and medicolegal consultant. He is the founder and CEO of RRS Education, a continuing education company providing weekly research reviews, informative seminars and convenient online courses for chiropractors, physiotherapists and osteopaths around the world. He has lectured as a part-time faculty member at the Canadian Memorial Chiropractic College in the Orthopedics Department for 13 years. For questions, contact shawn@rrseducation.com or to learn more about RSS Education, visit www.rrseducation.com.
References:
- Micheli S, Paciaroni M, Corea F, et al.: Cervical artery dissection: emerging risk factors. Open Neurol J 2010; 4: 50–55.
- Haneline MT, Lewkovich G. An analysis of the etiology of cervical artery dissections: 1994 to 2003. J Manipulative Physiol Ther 2005; 28: 617-622.
- Triano J, Kawchuk GN, eds. Current Concepts in Spinal Manipulation and Cervical Arterial Incidents. West Des Moines, IA: NCMIC Group Inc; 2005.
- French J, Gronseth G. Lost in a jungle of evidence: we need a compass. Neurology 2008; 71: 1634–1638.
Source:
![]()




{kind=link}