


By: Mark Charrette, DC
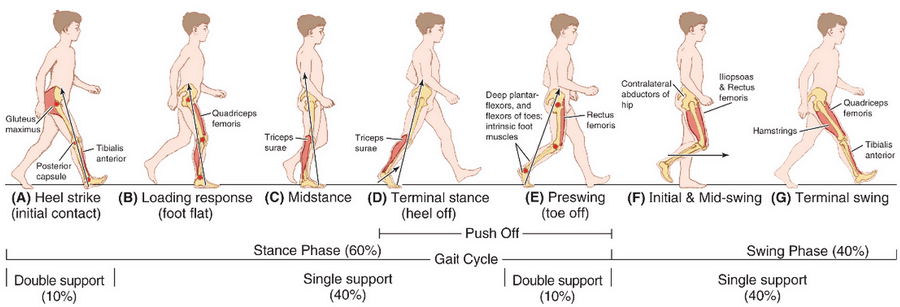
From the moment the heel strikes a surface, until the time the toes push off, a very predictable and complex series of motions occur. The Gait Cycle, as it is known, has two distinct portions, the Stance Phase, which is weight-bearing, and the Swing Phase, which is not.
Stance Phase
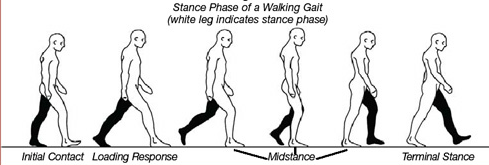 The Stance Phase, which comprises 60% of the gait cycle, begins when the heel strikes the ground. The force upon heel strike is equal to 2.5 times the body weight in a walking gait and 3.5 the body weight in a running gait. This is the equivalent of a 160-pound individual being hit in the head by 80 pounds with each step. In addition, the typical adult in today’s modern society takes at least 5,000 to 10,000 steps per day. Many individuals take as many as 14,000 steps per day. These repetitive shockwaves, that start at heel strike and can be measured at the cranium, occur on each step taken. The cumulative effect of these forces can cause the ligaments support the arches in the feet to stretch, in a permanent way, and cause various musculoskeletal symptoms in the lower extremity and spine to develop. Symptoms involving the joints of the feet, knees, hips, and low back are common.
The Stance Phase, which comprises 60% of the gait cycle, begins when the heel strikes the ground. The force upon heel strike is equal to 2.5 times the body weight in a walking gait and 3.5 the body weight in a running gait. This is the equivalent of a 160-pound individual being hit in the head by 80 pounds with each step. In addition, the typical adult in today’s modern society takes at least 5,000 to 10,000 steps per day. Many individuals take as many as 14,000 steps per day. These repetitive shockwaves, that start at heel strike and can be measured at the cranium, occur on each step taken. The cumulative effect of these forces can cause the ligaments support the arches in the feet to stretch, in a permanent way, and cause various musculoskeletal symptoms in the lower extremity and spine to develop. Symptoms involving the joints of the feet, knees, hips, and low back are common.
Heel Strike
The heels strikes lateral to the midline of the foot on the posterior and lateral aspect of calcaneus with the foot in a slightly supinated position. The leg is externally rotated upon heel strike. As weight is transferred anteriorly onto the foot, a pronation motion occurs where weight is transferred toward the medial aspect of the foot. This motion is accomplished mostly at the subtalar joint by combining eversion, dorsiflexion, and abduction. As this motion occurs, there is a collapse of the medial and lateral longitudinal arches and the navicular drops. As the navicular prominence drops in an inferior and medial direction, the metatarsals and toes move laterally. This will cause the foot to abduct or “toe-out.” Then the anterior and posterior tibialis muscles contract eccentrically to slow down the plantar flexion of the foot. When these muscles become overloaded and painful, it is known as “shin splints.”

Mid Stance
This is the portion of the stance phase where the heel and toes of the foot are both in contact with a surface. At mid stance or “foot flat” all three arches of the foot decrease their height creating a longer, wider, and flatter foot. One of the most common conditions of the foot is excessive or hyperpronation. In this condition, the constant forces generated at heel strike will create permanent stretching of the soft tissue retaining mechanism of the arches called Plastic Deformation. Structural support for the arches is primarily ligamentous from the plantar fascia and the spring ligament. The greatest degree of excessive pronation can be seen and measured in the functional foot (weight-bearing) at mid stance.
At mid stance, the tibia and femur are internally rotated maximally. These increased rotational forces are transmitted superior up the leg to the pelvis and specifically to the sacroiliac joint. Various pelvic subluxation complexes may develop such as pelvic tilting (usually anterior or to one side), and innominate rotations (usually posterior and inferior).
Neurologically, this will also cause an increase in nociceptive firing (type 4 mechanoreceptors), potentially creating a pain response in various tissues and adding to the reflexive activation of the sympathetic nervous system which creates a hyper-excitable central state in the body.
In cases of excessive or hyper pronation, more stress is put on the knee, especially the medial collateral ligament, the medial meniscus, and the anterior cruciate ligament at mid stance. When this occurs, symptomatology involving the medial aspect of the knee is common. Patellar tracking problems such as chondromalacia patellae can also occur.
Propulsion
This portion of the gate cycle is also known as Toe-Off. In this phase, the foot effectively becomes a lever. The posterior structures of the foot provide force as the ball of the foot serves as a fulcrum. This propulsion brings the foot away from the ground and launches it into the Swing Phase where no weight is borne until the next heel strike.
Swing Phase
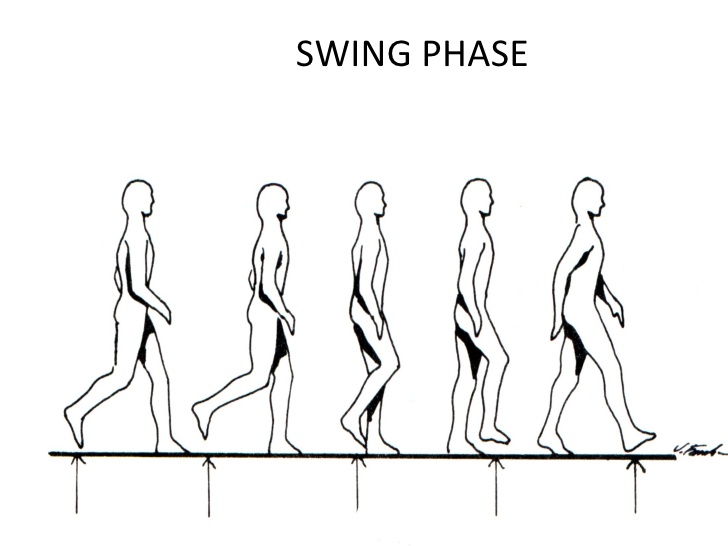
In the swing phase of the gate, the pelvis rotates forward and the hip flexes, this accelerates the leg forward. Muscles contract concentrically pulling the body forward. The knee and ankle complex flex to clear the ground, then they extend in order for the heel to strike on its’ posterior lateral aspect.
Leg Length Inequality
Excessive or hyper pronation will create a functional inequality of leg lengths. This will affect muscular tension and the amount of weight born by various joints. Strain on the body increases and endurance may be reduced so that routine movements will require greater muscular effort and cause fatigue. Pain and discomfort are common responses. Since the nature of pronation is usually bilateral and asymmetrical this type of pedal foundation can  create pelvic tilting and/or rotation.
create pelvic tilting and/or rotation.
So, it appears that bilateral and asymmetrical excessive pronation is developed slowly and in order to have a balanced lower extremity and spine the 3 arches of the feet and the subtalar joint must be stabilized to allowed for normal ranges of motion and block excessive motion.
This post was sponsored by the #1 Foot Orthotic Company in Chiropractic: Foot Levelers
References
- Aota Y, Iizuka H, Ishige Y, et al. Effectiveness of a lumbar support continuous passive motion device in the prevention of low back pain during prolonged sitting. Spine. 2007;32(23):E674-7.
2 Boswell MV, Shah RV, Everett CR, et al. Interventional techniques in the management of chronic spinal pain: evidence-based practice guidelines. Pain Physician, 2005;8(1):1-47.
- Furman and Gallo, 2000. The Neurophysics of Human Behavior.
- Patterson M. The spinal cord: participant in disorder.
J Spinal Manip: 1993:9(3)2-11
- Langer S. (1976) Structural Leg Syndrome. JAPA66:723.
- Huang et al: Biomechanical Evaluation of Longitudinal Arch Stability. Foot & Ankle, Vol. 14, No. 6, July/August 1993
- Basmajian JV et al.The Role of Muscles in Arch Support of the Foot: An Electromyographic Study. J of Bone and Joint Surgery, Vol 45, No 6 September 1963.
- Gould N. Evaluation of hyperpronation and pes planus in adults. Clin Orthop 1983; 181:37-45
- Magee DJ. Orthopedic physical assessment. 2nd ed. Philadelphia: WB Saunders, 1992:459

Dr. Mark Charrette is a 1980 summa cum laude graduate of Palmer College of Chiropractic in Davenport, Iowa. He is a frequent guest speaker at twelve chiropractic colleges and has taught over fourteen hundred seminars worldwide on extremity adjusting, biomechanics, and spinal adjusting techniques. His lively seminars emphasize a practical, hands-on approach.
Dr. Charrette is a former All-American swimmer, who has authored a book on extremity adjusting and also produced an instructional video series. Having developed succesful practices in California, Nevada, and Iowa, Dr. Charrette currently resides in Texas.




{kind=link}